
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Early Identification of Patients with Multiple Myeloma Progressing within a Short-Term following Tandem Transplantation
.jpg "Tongyong Yu, Doctor photo")
Tongyong Yu, Doctor
post-doctor
The first affiliated hospital of Sun Yat-sen University
High-dose chemotherapy followed by autologous stem cell transplant (ASCT) remains the standard treatment for transplant-eligible patients with newly diagnosed multiple myeloma (MM), significantly improving long-term outcomes. Tandem ASCT, defined as a second ASCT within six months of the initial procedure, has been proposed to further optimize therapeutic efficacy. However, early disease progression following tandem ASCT remains a significant challenge, reflecting the inherent biological heterogeneity of MM. In this study, we identified that patients progressing within 12 months post-tandem ASCT demonstrated markedly inferior progression-free survival (PFS) and overall survival (OS) compared to who did not progress within 12 months. In this study, we aim to explore risk factors associated with clinical features to identify these high-risk patients and construct a prognostic model. This model may facilitate early risk stratification and therapeutic optimization for high-risk patients in clinical practice.
Methods:
This retrospective cohort study analyzed consecutively enrolled patients with newly diagnosed MM undergoing tandem ASCT between July 1, 2017, and March 31, 2025, with a second transplantation follow-up duration ≥12 months. The cohort was randomly allocated into training (n=23, 70%) and validation (n=11, 30%) sets. Univariate and multivariate analyses were performed to identify independent risk factors for patients progressing within 12 months post-tandem ASCT. A prognostic nomogram was developed using logistic regression algorithms and internally validated.
Results:
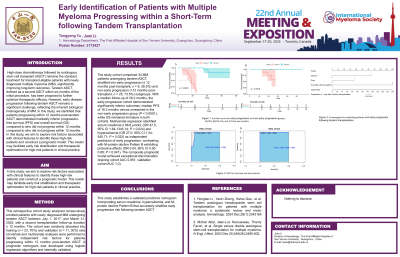
The study cohort comprised 34 MM patients undergoing tandem ASCT, stratified into early progression (≤12 months post-transplant, n=9, 26.5%) and non-early progression ( >12 months post-transplant, n=25, 73.5%) subgroups. With a median follow-up of 26.2 months, the early progression cohort demonstrated significantly inferior outcomes: median PFS of 18.3 months versus unreached in the non-early progression group (P < 0.0001), while OS remained immature in both cohorts. Multivariate regression identified serum creatinine ≥ 96.8 μmol/L (OR 47.0, 95% CI 1.64-1345.14; P = 0.024) and hypercalcemia (OR 27.0, 95% CI 1.34-545.71; P = 0.032) as independent predictors of early progression, contrasting with M-protein decline Pattern B exhibiting protective effects (OR 0.04, 95% CI 0.00-0.88; P = 0.041). The composite prognostic model achieved exceptional discrimination (training cohort AUC 0.951; validation cohort AUC 1.0).
Conclusions: This study establishes a validated predictive nomogram incorporating serum creatinine, hypercalcemia, and M-protein decline Pattern B that accurately stratifies early progression risk following tandem ASCT.