
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
Circulating plasma cells evaluation before and after CAR T-cell therapy as a dynamic factor for response assessment
 photo")
Federico Monaco, MD (he/him/his)
Medical Doctor
A.O.U. SS. Antonio e Biagio e Cesare Arrigo
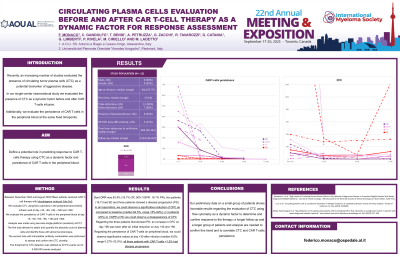
Recently, an increasing number of studies evaluated the presence of circulating tumor plasma cells (CTC) as a potential biomarker of aggressive disease. In our single-center observational study we evaluated the presence of CTC as a dynamic factor before and after CAR T-cells infusion in order to define a potential role in predicting response to the therapy. Additionally, we evaluate the persistence of CAR T-cells in the peripheral blood at the same fixed timepoints to underline a possible correlation.
Methods:
Between December 2024 and May 2025 nine patients underwent lymphocyte apheresis and received CAR T-cell therapy with Idecabtagene vicleucel (Ide-Cel). We plan to evaluate CTC using flow cytometry (FC) in the peripheral blood before infusion, at day +30, +60, +90, +180 and +360 after infusion; similarly we evaluate the persistence of CAR T-cells in the peripheral blood at day +6, +30, +60, +90, +180 and +360 after infusion. Regarding CTC, the analysis was made using two-tube single-platform (sensitivity 4x10–6). The first tube allowed to select and quantify the absolute count of plasma cells (PC) and identify those with abnormal phenotype. Thereafter, PC were identified by CD38/CD138 gate (CD38+/CD138+) and pathologic PC by specific expression at diagnosis. Similarly, a second tube with intracellular antibody combination was performed to assess and confirm the CTC clonality. The threshold for CTC detection was defined as 20 PC events out of 5.000.000 events analyzed. Multiple Myeloma serological response was evaluated as for IMWG response criteria.
Results:
We analyzed eight out of nine patients; one patient was excluded from the analysis for early death before day +30 after infusion. In all eight patients analyzed (100%) CTC were detected by FC at baseline. Median follow-up was 77 days after infusion, the best ORR was 87.5% (37.5% RP, 50% VGPR), one patient (12.5%) showed progressive disease (PD) at day +90. In all 7 patients that reached a response, we could observe a significative reduction of CPC as compared to baseline (median 79.5%, range 32.65%-100%); in 2 patients (25%) in VGPR we could observe a disappearance of CPC (values < 20 PC events out of 5.000.000 events analyzed). Regarding the patient that showed PD an increase in CPC on day +90 was seen after an initial reduction on day +30 and +60. Regarding the persistence of CAR T-cells on peripheral blood, we could observe significative values at day +30 after infusion (median 14.8%, range 0.75%-58.5%); the only patient with CAR T-cells < 1% was the one that shows disease progression at day +90.
Conclusions:
In conclusion, our preliminary data on this group of patients shows favorable results regarding the evaluation of CTC using flow cytometry as a dynamic factor to determine and confirm response to the therapy; a longer follow-up and a larger group of patients and analysis are needed to confirm this trend and to correlate CTC and CAR T-cells persistence.