
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
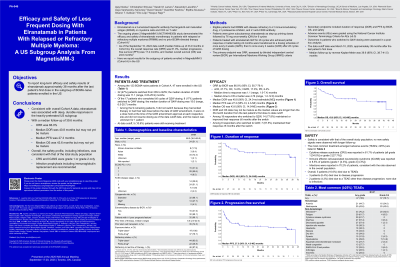
Efficacy and Safety of Less Frequent Dosing With Elranatamab (ELRA) in Patients With Relapsed or Refractory Multiple Myeloma (RRMM): A US Subgroup Analysis from MagnetisMM-3
.jpg "Ajay K. Nooka, MD, MPH, FACP (he/him/his) photo")
Ajay K. Nooka, MD, MPH, FACP (he/him/his)
Professor, Director of Myeloma Program
Winship Cancer Institute of Emory University
Eligible pts had RRMM with disease refractory to ≥1 immunomodulatory drug, ≥1 proteasome inhibitor, and ≥1 anti-CD38 antibody. Pts were given subcutaneous ELRA as step-up priming doses followed by 76 mg QW for 6 cycles. Pts given QW dosing for ≥6 cycles who achieved partial response or better lasting ≥2 mo were transitioned to Q2W dosing and to Q4W after ≥6 cycles of Q2W dosing. The subgroup of pts within Cohort A enrolled in the US (n=47) was analyzed. At data cutoff (March 10, 2025 [≈38 mo after last pt first dose]), median follow‐up was 39.6 mo (95% CI, 38.7-41.5; estimated by reverse Kaplan–Meier).
Results:
Pts in the US subgroup had a median of 5 prior lines of therapy (range, 2-22); 93.6% were triple-class refractory, and 46.8% were penta-drug refractory. Eight (17.0%) pts were Black or African American. ORR (95% CI) by Blinded Independent Central Review was 66.0% (50.7-79.1); 42.6% of pts achieved complete response (CR) or better. Median (range) time to response was 1.08 mo (0.95-7.36), and median time to CR or better was 4.76 mo (1.22-12.75). Median duration of response (95% CI) was 40.8 mo (24.0-not estimable [NE]). Median (95% CI) PFS and OS were 27.3 mo (4.3–NE) and 43.6 mo (14.9–NE), respectively. Median DOR and OS were after 38 mo and potentially not yet mature. Any grade [G] and G3/4 treatment-emergent adverse events were reported in 100% and 78.7% pts, respectively. Infections (any G, G3/4, G5) were reported in 70.2%, 42.6%, and 0.0%, respectively; 51.1% received Ig replacement. Anti-viral, anti-pneumocystis jirovecii pneumonia, anti-bacterial, and anti-fungal prophylaxis were received by 80.9%, 23.4%, 14.9%, and 8.5% of pts, respectively. The rate of cytokine release syndrome (CRS) was 61.7% (G1, 34.0%; G2, 27.7%; G≥3, 0.0%). Immune effector cell-associated neurotoxicity syndrome was reported in 8.5% of pts (G1, 4.3%; G2, 4.3%; G≥3, 0.0%). 22 pts switched from QW to Q2W, and 8 pts further switched from Q2W to Q4W dosing
Conclusions:
Pts with RRMM in MagnetisMM-3 Cohort A, including the US subgroup, were heavily pretreated. Consistent with overall Cohort A data, ELRA induced deep, durable responses in the US subgroup, with a mPFS of 27.3 mo. CRS was G1 and G2 only. Infections were consistent with what was observed in the overall study population; infection prophylaxis including Ig replacement are recommended.