
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Outcomes and Maintenance Strategies for Transplant-Eligible Newly Diagnosed Multiple Myeloma Among Patients Age 40 and Younger
 photo")
Arvind Suresh, MD (he/him/his)
Resident Physician
Division of Hematology/Oncology, University of California San Francisco
The median age at diagnosis for multiple myeloma is approximately 70 years old, and < 2% of patients are age ≤40 at diagnosis. Although younger patients may have better tolerance to therapies, there may be greater impacts on quality of life (QoL) and late toxicities of therapies. Disease characteristics and outcomes are also less well-described in this group. We explored outcomes and maintenance strategies for patients age ≤40 with transplant-eligible newly diagnosed multiple myeloma (NDMM).
Methods:
We conducted a single center retrospective analysis of patients who underwent autologous stem cell transplantation (ASCT) for NDMM between 2004-24 and identified patients who were diagnosed and underwent ASCT at age ≤40. Demographic and disease features were analyzed using descriptive statistics. Survival outcomes were analyzed using the Kaplan-Meier method. Univariate and multivariate analysis was conducted using a Cox regression model to identify predictors of survival.
Results:
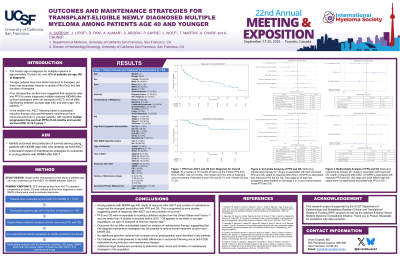
We identified 54 out of 1512 patients (3.6%) who underwent ASCT for NDMM at age ≤40, with a median age of 37 years (range 28-40). 44.4% of patients were male and 22.2% identified as Hispanic/Latino. 44.4% of patients identified as white, 13% as Asian, and 11.1% as Black. 68.5% had heavy chain disease and 22.7% had ISS stage 3 disease. 27.1% had ≥1 high-risk cytogenetic abnormality and 16.7% met 2024 IMWG high-risk criteria. Two patients received a tandem ASCT. At a median follow-up duration of 106 months, the median progression-free survival (PFS) after ASCT was 53 months (range 28-117). Median overall survival (OS) was not reached with an estimated 5-year OS of 85.1% and 10-year OS of 71.5%. Eight patients received consolidation after ASCT and 45 received maintenance therapy with a median duration of 15 months (range 0-148). On univariate analysis, longer duration of maintenance therapy had a minimal impact on PFS (HR 0.99, p=0.04), while multi-drug maintenance was associated with improved PFS (HR 0.30, p=0.01) and OS (HR 0.11, p< 0.005). Patients not started on any maintenance therapy had worse PFS (HR 3.34, p=0.006) and OS (HR 9.33, p< 0.001). Presence of high-risk cytogenetics had a trend toward worse PFS (HR 1.74, p=0.19). On multivariate analysis, depth of response after ASCT was associated with improved PFS but only the number of maintenance drugs was associated with improved OS (HR 0.23, p=0.03). Three patients developed secondary malignancies, 1 with T-cell lymphoma and 2 with t-AML.
Conclusions:
Among patients with NDMM age ≤40, depth of response after ASCT and number of maintenance drugs had the strongest association with PFS and OS. PFS and OS were comparable to previously published studies. Outcomes did not differ based on duration of maintenance therapy, suggesting that risk-adapted maintenance strategies may be possible to reduce overall treatment duration and benefit QoL. Additional studies are warranted to determine ideal choice and duration of maintenance strategies in this population.