
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
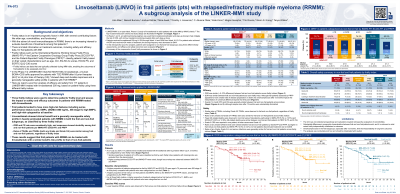
Linvoseltamab (LINVO) in frail patients (pts) with relapsed/refractory multiple myeloma (RRMM): A subgroup analysis of the LINKER-MM1 study
 photo")
Hira Mian, MD (she/her/hers)
Associate Professor
McMaster University, Hamilton, ON, Canada
Bispecific antibodies (bsAbs) are a significant advancement for certain pts with MM. Frailty is known to be a key indicator of pt prognosis and impacts the efficacy and toxicities of MM therapy. Currently, data are limited on how frailty impacts outcomes for pts treated with bsAbs. In LINKER-MM1 (NCT03761108) LINVO, a human BCMA×CD3 bsAb approved in the EU, showed high response rates with a generally manageable safety profile in pts with RRMM. We report efficacy and safety from LINKER-MM1 based on frailty status.
Methods:
Pts with triple-class exposed RRMM received LINVO IV QW through Week 14–16 (step-up dosing in Week 1–2), then Q2W. Phase 2 pts who had ≥VGPR and received ≥24 weeks of LINVO 200 mg switched to Q4W dosing. Frailty was evaluated post hoc using three different indices: ECOG Proxy Frailty (ECOG-PF) score, International Myeloma Working Group Frailty Proxy (IMWG-FP), and Patient-Reported Frailty Phenotype (PRFP) measure (Facon et al. Leukemia 2020; Murugappan et al. J Geriatr Oncol 2024). Objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and tx-emergent AEs (TEAEs) were assessed by frailty status per IMWG-FP and PRFP.
Results:
As of 23 July, 2024, 117 pts were enrolled into the 200 mg cohorts (median [m] follow-up: 21.3 months [mo]). There was variation among the different scores in classifying patients as frail. By IMWG-FP, 32 frail and 77 non-frail; and by PRFP, 24 frail and 89 non-frail. Differences in baseline characteristics were seen among frail and non-frail pts across all indices. For example, frail vs non-frail pts were older by IMWG-FP (m 75 vs 65 years), but not PRFP (68 vs 71 years); a greater proportion of frail vs non-frail pts had ECOG PS 1 (IMWG-FP: 91 vs 66%; PRFP: 88 vs 70%) and higher tumor burden (sBCMA ≥400 ng/mL; IMWG-FP: 66 vs 36%; PRFP: 54 vs 42%).
Responses were generally high among frail and non-frail pts; ORRs in frail and non-frail pts were 66% and 73% by IMWG-FP and 63% and 73% by PRFP, respectively. mPFS (95% CI) for frail vs non-frail pts by IMWG-FP was not reached (NR; 3.3 mo–non-evaluable [NE]) vs NR (17.3 mo–NE); and by PRFP, 17.3 mo (11.8–NE) vs NR (19.7 mo–NE). mOS (95% CI) for frail vs non-frail pts by IMWG-FP was 27.8 mo (13.0–NE) vs NR (23.8 mo–NE); and by PRFP, 23.8 mo (13.0–NE) vs NR (31.4 mo–NE).
Grade 3/4 TEAEs were consistent across frail and non-frail pts (IMWG-FP: 75% and 73%, respectively; PRFP: 71% and 74%, respectively). Grade 3/4 CRS, ICANS, and infections in frail and non-frail pts ranged 0–4.2%, 1.1–8.3%, and 35–42%, respectively, across frailty measures.
Conclusions:
Overall, efficacy and safety of LINVO 200 mg was consistent in frail and non-frail pts, with high responses, durable OS/PFS, and a generally manageable safety profile regardless of frailty status index. These results suggest that frail, older adults can be treated with LINVO with a similar risk-benefit profile to non-frail patients. Efficacy and safety per ECOG-PF score will be presented at the meeting.