
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
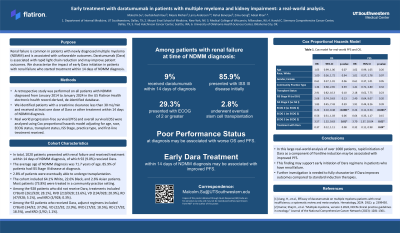
Early treatment with daratumumab in patients with multiple myeloma and kidney impairment: a real-world analysis.

Malcolm Su, MD
Resident Physician
UTSW
Renal failure is common in patients with newly diagnosed multiple myeloma (NDMM) and is associated with unfavorable outcomes. Daratumumab (Dara) is associated with rapid light chain reduction and may improve patient outcomes. We hypothesized that, among patients with kidney impairment who started treatment within 15 days of NDMM diagnosis, early Dara initiation would be associated with improved outcomes.
Of 1946 patients with NDMM and initial CrCl< 45 mL/min, 175 (9.0%) received at least one dose Dara within 15 days of NDMM diagnosis. The mean (SD) age at diagnosis was 72.5 (10.1) years, with 762 (72.8%) presenting with ISS Stage III disease and 61 (3.1%) eventually able to receive stem cell transplantation. Among the 1771 patients who did not receive Dara, treatments included CYBorD (21.0%), RVD (30.1%), VD (18.6%), KRD (0.7%), RD (7.8%), and dexamethasone alone (3.8%). Among the 175 patients who received Dara, adjunct regimens included CYBorD (17.7%), RVD (19.4%), VD (19.4%), KRD (0.6%), RD (18.3%), and dexamethasone (2.9%).
Patients with baseline CrCl < 45 mL/min receiving Dara had improved rwPFS (log-rank p=0.03) compared to non-Dara recipients; there was no difference in rwOS (log-rank p=0.3). The median rwOS and rwPFS were 37.1 and 20.4 months, respectively. After adjusting for confounders, the association between Dara with rwPFS was attenuated (p=0.1). In contrast, lower ECOG status and younger age were associated with improved rwPFS and rwOS.
In total, 1020 (52.4%) patients presented with CrCl < 30 mL/min, of which 92 (9.0%) received Dara. In patients with baseline CrCl < 30 mL/min, there were no apparent differences in rwPFS (p=0.8) or rwOS (p=0.9) between Dara and non-Dara recipients. The median rwOS and rwPFS were 35.2 and 19.2 months, respectively. After adjusting for confounders, treatment with Dara was associated with improved rwPFS (p=0.04) and rwOS (p=0.08). Lower ECOG status was also associated with improved rwPFS and rwOS.
In this large real-world analysis, rapid initiation of Dara as a component of frontline induction was associated with improved rwPFS among patients with CrCl < 30 mL/min. This finding may support the early initiation of Dara regimens in renal failure. Further investigation is needed to fully characterize if Dara improves outcomes compared to standard induction therapies.