
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Impact of Cumulative and Relative Dose Intensity of Bortezomib, Lenalidomide, and Dexamethasone (VRD) on Depth and Duration of Response in Newly Diagnosed Multiple Myeloma (MM)
 photo")
Anna Moreno Cosialls (she/her/hers)
Hematologist
Institut Català d'Oncologia (ICO) Badalona-Hospital Germans Trias i Pujol, Badalona.
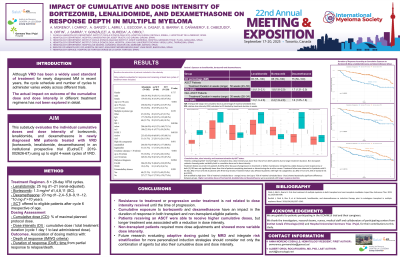
Although VRD is a widely used standard of treatment for newly diagnosed MM, the cycle schedules and number of cycles to administer vary across different trials. The actual impact on outcome of the cumulative dose and dose intensity in different treatment regimens has not been explored in detail. This substudy evaluates the individual cumulative doses and dose intensity of bortezomib, lenalidomide, and dexamethasone in newly diagnosed MM patients treated with VRD (bortezomib, lenalidomide, dexamethasone) in an institutional prospective trial (EudraCT: 2019-002626-67) using up to eight 4-week cycles of VRD.
Methods:
The trial recruited 360 patients with newly diagnosed MM across several centres from a single institution. Individuals with full dosing information, receiving at least 8 weeks of treatment and two or more treatment cycles (N=304; 84%) were eligible for this substudy. VRD schedule consisted of 8 cycles of lenalidomide (len) 25 mg/day 21/28 (adjusted if renal insufficiency), bortezomib (btz) 1.3 mg/m2 days 1,4,8,11 and dexamethasone (dex) 20 mg days 1,2,4,5,8,9,11,12 (half dose for patients > 70 years). Irrespective of age, autologous stem cell transplantation (SCT) was offered to patients considered eligible and was performed after cycle 6. Dosing data for bortezomib, lenalidomide, and dexamethasone included the cumulative dose across all cycles and were expressed as percent of maximal dose per schedule, dose intensity was calculated as the dose of each individual drug divided by the total duration of the 8 cycle treatment. We evaluated the association of cumulative doses and dose intensities with depth of response per IMWG criteria and duration of response (DoR) defined as time from partial response to relapse or death from any cause.
Results:
Patients age ranged from 31 to 88 years old (median 62) and 166 were male (55%), 18% had a creatinine clearance < 30 ml/min. Mean treatment duration was 47.5 weeks (for patients receiving SCT) and 29.7 weeks (non-SCT). Older patients ( >70 years) received significantly lower cumulative doses of all drugs, btz 72% (Standard Deviation 23) vs 83% (SD 21), len 60% (SD 28) vs 78% (SD 26) and dex 39% (SD 13) vs 77% (SD 25), p< 0.0001 all comparisons. Partial response or better was achieved in 299/304 cases (98%), Cumulative doses below 75% of btz, len or dex were all associated with lower probabilities of achieving VGPR or better, 75 vs 91%, 82 vs 89% and 80 vs 93% for btz, len and dex respectively (p< 0.001 all comparisons). Median DoR was 5 years and cumulative doses below 75% were again associated to shorter DoR (p< 0.001).
Conclusions:
Dose reductions of btz, len or dex below 75% expected cumulative dose were associated wih lower rates of CR and shorter duration of response. Our findings highlight the critical relevance of treatment optimization and toxicity management to maintain full induction treatment.