
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Efficacy and Safety of Bortezomib, Pomalidomide and Dexamethasone (VPD) in Newly Diagnosed Multiple Myeloma: Single-arm, Phase-II Investigator Initiated Prospective Clinical Trial
 photo")
Jeevan Kumar, MD, DrNB Hematology (he/him/his)
Senior Consultant
Tata Medical Center, Kolkata, India
A total 50 patients were enrolled between April 2020 to March 2024. Median follow up was 27.3 months (range 9.0-59.6 months). The median age was 58 years (38-71), and gender ratio was 1:1. High risk cytogenetics were seen in 50.0% (n 25) patients. According to revised international staging system for myeloma (RISS) stage I, II and III were present in 12% (n 6), 50% (n 25) and 38% (n 19) of patients respectively.
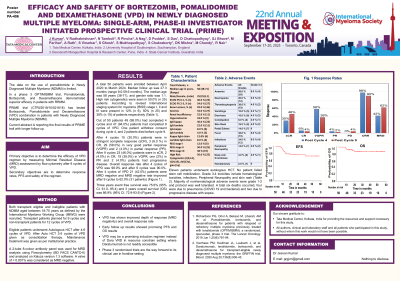
Out of 50 patients 49 (98.0%) had completed 4 cycles and 47 (94.0%) patients had completed 9 cycles of VPD. After 4 cycles 15 (30.0%) patients were in stringent complete response (sCR), 3 (6.0 %) patients in CR, 29 (58.0%) in very good partial response (VGPR) and 2 (4.0%) in partial response (PR). After 9 cycles 23 (46.0%) patients were in sCR, 2 (4.0%) in CR, 19 (38.0%) in VGPR, one (2%) in PR and 2 (4.0%) patients had progressive disease. Overall response rate after 4 cycles of VPD was 98.0% and after 9 cycles was 90.0%. After 4 cycles of VPD 21 (42.0%) patients were MRD negative and MRD negative rate improved after 9 cycles to 62.0% (31 patients). Three years event free survival was 75.6% (95% CI: 61.0- 85.4) and 3 years overall survival (OS) was 86.9% (95% CI: 72.9-93.9).
Eleven patients underwent auto HCT. No patient failed stem cell mobilization. Grade 3-4 toxicities include hematological toxicities (10%), infections (10%) and skin rash (4%). Majority of nonhematological adverse events were grade 1 to 2 and protocol was well tolerated. A total six deaths occurred, four were due to pneumonia (COVID 19 and bacterial) and two due to progressive disease with sepsis.
Conclusions: VPD has shown improved depth of response (MRD negativity) and overall response rate. Early follow up results showed promising PFS and OS results. VPD may be a promising induction regimen instead of Dara VRD in resource constrain setting where Daratumumab is not readily accessible. Phase 3 randomized trials are the way forward to its clinical use in frontline setting.