Introduction: Waldenstrom Macroglobulinemia is a type of IgM-secreting lymphoplasmacytic lymphoma marked by frequent mutations in MYD88 and CXCR4. WM-associated AL Amyloidosis (WM-AL) is a relatively unexplored clinical entity, with little data on survival outcomes, treatment regimens and prognostic factors. This is distinct from typical AL Amyloidosis that is classically associated with Plasma Cell Dyscrasias.
Methods: We conducted a retrospective observational study of adults with Waldenstrom Macroglobulinemia-associated cardiac AL amyloidosis (WM-AL) at Cleveland Clinic from January 2012 to December 2022. Patients diagnosed with other amyloidosis types or incomplete clinical data were excluded. Demographic details, diagnostic labs, treatments, and responses were collected from medical records. Categorical variables were presented as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges (IQR).
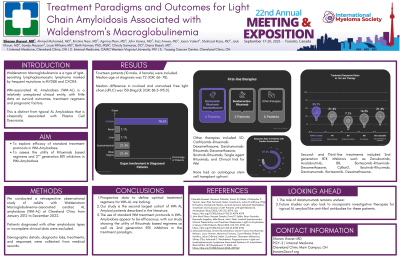
Results: Fourteen patients (10 male, 4 female) were included. Median age at diagnosis was 72 (IQR: 66- 78). Organ involvement included cardiac (78.6%), renal (7.1%), liver (7.1%), gastrointestinal (21.4%), and other organs (21.4%) including soft tissue and peripheral nerve. Median difference in involved and uninvolved free light chain (dFLC) was 150.8mg/dL (IQR: 86.5-193.0). A median of 1 (IQR;1-3) line of therapy was delivered after the diagnosis of WM-AL was made. Patients were mainly treated with the following first-line therapies: Bortezomib-Rituximab- Dexamethasone in 6 (42.9%), Bendamustine-Rituximab (BR) in 2(14.2%). The remaining patients each received one of the following regimens: VD, Carfilzomib-Rituximab-Dexamethasone, Daratumumab-Rituximab-Dexamethasone, Ibrutinib-Rituximab, Single agent Rituximab, and Clinical trial for WM. None had an autologous stem cell transplant upfront. Second- and Third-line treatments included 2nd generation BTK inhibitors such as Zanubrutinib, Acalabrutinib, BR, Bortezomib-Rituximab-Dexamethasone, CyBorD, Ibrutinib-Rituximab, Daratumumab- Bortezomib- Dexamethasone.
In response to 1st line treatment, 35.7% achieved a VGPR or better, 21.4% PR, 7.1% had PD, 14.3% had NR, and 21.4% were not evaluable. Of patients with cardiac involvement, 87.5% of them achieved a cardiac response.
Conclusions: Prospective data to define optimal treatment regimens for WM-AL are lacking, but our study is the second largest cohort of WM AL Amyloid patients described in the literature. The use of standard WM treatment protocols in WM-Amyloidosis appear to be efficacious, with our study showing the utility of Rituximab based regimens as well as 2nd generation BTK inhibitors in the treatment paradigm. The role of daratumumab remains unclear. Future studies can also look to incorporate investigative therapies for typical AL amyloid like anti-fibril antibodies for these patients.