
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
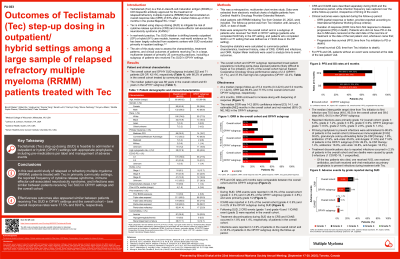
Outcomes of Teclistamab (Tec) step-up dosing in outpatient/hybrid settings among a large sample of relapsed refractory multiple myeloma (RRMM) patients treated with Tec

Binod Dhakal, MD, MS
Associate Professor/Hematologist
Medical College of Wisconsin
This was a retrospective, multicenter chart review study. Data were extracted from electronic medical charts of eligible pts from a large oncology provider network. Adult pts with RRMM initiating Tec since FDA approval (10/25/22) were included. Characteristics and treatment history were captured during the baseline period; cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), and infections were captured during the treatment period; and clinical outcomes were captured during the follow-up period. Variables were analyzed in all included pts and in a subgroup of OP/HY pts (i.e., who completed SUD fully in OP setting or had ≥1 SUD dose in the OP setting).
Results:
The overall cohort and OP/HY SUD subgroup included 222 and 71 pts (29 OP, 42 HY), respectively, with 66% of all pts treated by community providers. The overall cohort had a median age of 68 years, with 60% male, 75% White and 19% Black (OP/HY SUD: median age 63 years, 61% male, 78% White and 18% Black). At Tec initiation, 37% of the overall cohort had R-ISS stage III disease (OP/HY: 27%), 77% had an ECOG score of 0-1 (OP/HY: 78%), 38% had high-risk cytogenetics (OP/HY: 42%), and 95% were triple-class exposed (OP/HY: 93%). Median prior lines of therapy were 4 in both the overall cohort and OP/HY subgroup. During SUD, CRS occurred in 33% (highest grade (G) 1: 21%, G2: 10%, G3: 2%) of all pts and 27% (G1: 16%, G2: 9%, G3: 3%) of OP/HY pts; ICANS occurred in 5% (highest G1: 3%, G2: 2%, G4: 1%) of all pts and 4% (G1: 3%, G2: 1%) of OP/HY pts. Primary prophylaxis for infections was administered to 81% of all pts and 72% of OP/HY pts. At a median follow-up of 5.4 months, infections occurred in 15% (highest G1: 6%, G2: 7%, G3: 1%, G5: 1%) of all pts and 18% (G1: 9%, G2: 6%, G3: 3%, G5: 1%) of OP/HY pts during Tec treatment. Treatment discontinuations due to CRS, ICANS and infections occurred in 2%, 1%, and 2% of all pts, respectively. The overall response rate (ORR) was 70% in all pts and 78% in OP/HY pts.
Conclusions:
In this RW study of pts treated with Tec in primarily community settings, safety (CRS, ICANS, infections) and effectiveness (ORR) outcomes appeared comparable between pts receiving Tec SUD in OP/HY settings and the overall cohort, demonstrating that it is feasible to administer Tec SUD in OP/HY settings with focus on appropriate prophylaxis and management.