
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
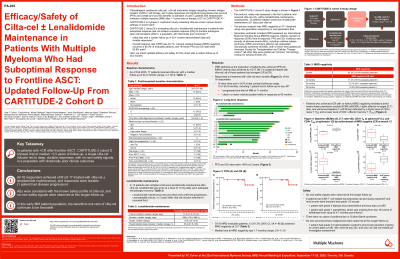
Efficacy/Safety of Cilta-cel ± Lenalidomide Maintenance in Patients With Multiple Myeloma Who Had Suboptimal Response to Frontline ASCT: Updated Follow-Up From CARTITUDE-2 Cohort D
 photo")
Yaël C. Cohen, MD (she/her/hers)
Head the Myeloma unit
Tel-Aviv Sourasky (Ichilov) Medical Center
CARTITUDE-2 (NCT04133636) is a phase 2 multicohort study evaluating ciltacabtagene autoleucel (cilta-cel) across various clinical settings. Cohort D is evaluating cilta-cel ± lenalidomide (len) maintenance in patients (pts) who achieved < complete response (CR) after autologous stem cell transplant (ASCT) frontline therapy (tx). We report updated efficacy and safety for this cohort with a longer median follow-up (mFU) of 40.2 mo.
Methods: Adults with newly diagnosed MM per IMWG criteria; best response of < CR and ≥stable disease after 4–8 cycles of initial tx, including induction, high-dose chemotherapy, and ASCT ± consolidation, and without exposure to CAR-T or anti-BCMA tx received a single cilta-cel infusion 5–7 d post lymphodepletion. Per protocol, safety was assessed in the first 5 pts who received cilta-cel only, without len maintenance; subsequently, 12 pts initiated continuous len maintenance ≥21 d post cilta-cel. Primary endpoint was MRD-negative rate at 10–5 based on next-generation sequencing or flow.
Results: As of Feb 2025 (mFU, 40.2 mo [range, 4.7–55.9]), 17 pts received cilta-cel (without len maintenance, n=5; with len maintenance, n=12). Median age was 54.0 yrs and 17.6% had high-risk cytogenetics at baseline. Compared with the previous report (22-mo mFU), ORR and rate of ≥CR were unchanged (16/17, 94.1% [95% CI, 71.3–99.9]; 1 pt withdrew consent at 4.7 mo with response not evaluable). 14/16 pts were alive in ≥CR (87.5%, [95% CI, 61.7–98.5]) at last contact (follow-up range, 13.4–55.9 months); 1 pt progressed and died of MM at 11 mo, and 1 pt died in a motor vehicle accident while in response at 42 mo. Overall, of 16 MRD-evaluable pts, 13 (81.3%, [95% CI, 54.4–96.0]) achieved MRD negativity at 10–5 at any time; median time to MRD negativity was 1.7 mo (range, 0.9–11.5). MRD-negative ≥CR rate was 71.4% at 12 mo (95% CI, 41.9–91.6; 10/14 evaluable pts), 72.7% at 24 mo (95% CI, 39.0–94.0; 8/11 evaluable), and 75.0% at 36 mo (95% CI, 34.9–96.8; 6/8 evaluable). Pts with MRD negative ≥CR were characterized by a trend toward lower pre-infusion sBCMA, higher effector-to-target ratio (peak expansion over pre-infusion sBCMA), and enhanced T cell fitness (ie, higher level of naive T cells and lower level of effector memory T cells). 6 pts had CAR-T cell related neurotoxicities; most events were low grade and transient except 1 with grade 3 diplopia (recovered) and 1 with grade 1 paresthesia ongoing from d 18 at the time of withdrawal from study at 4.7 mo post infusion. There were no cases of parkinsonism or Guillain-Barré syndrome, and no new safety signals were observed.
Conclusions:
In pts who had < CR after frontline ASCT, a single cilta-cel infusion ± len maintenance led to deep and durable responses, with no new safety signals at this longer follow-up. The efficacy and safety of cilta-cel in cohort D continues to be favorable, especially given the historically poor clinical outcomes seen for these pts.