
Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
Category: Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
Intravenous Immunoglobulin 10% as Primary Versus Secondary Infection Prophylaxis in Adults with Multiple Myeloma Receiving B-Cell Maturation Antigen×CD3-Directed Bispecific Antibody: A Phase 3 Trial

Guido Lancman, MD, M.Sc.
Assistant Professor and Myeloma Physician
University of Toronto, Princess Margaret Cancer Centre
Patients (pts) with multiple myeloma (MM) receiving B-cell maturation antigen (BCMA)×CD3-directed bispecific antibody (BsAb) therapy are at risk of severe infection, owing to both the underlying disease and its treatment. We aim to assess the efficacy, safety and tolerability of intravenous immunoglobulin (IVIG 10%) as primary vs secondary infection prophylaxis in pts with MM receiving BCMA×CD3-directed BsAb therapy.
Methods:
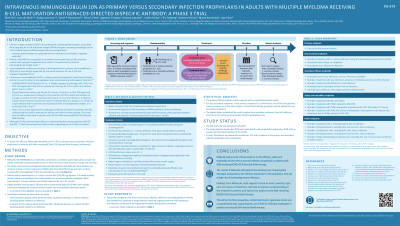
This multicenter, randomized, controlled, open-label phase 3 study is planned to be conducted in North America, South America, Europe and Asia Pacific. Eligible pts must be aged ≥18 years with a documented diagnosis of MM, have recently commenced teclistamab (within 8 weeks), have not received immunoglobulin treatment within 16 weeks before screening and have given informed consent. Exclusion criteria include an Eastern Cooperative Oncology Group performance status score of >2, documented polyclonal immunoglobulin G < 150 mg/dL at the most recent assessment within 4 weeks before starting teclistamab, current serious infection or >1 serious infection within 3 months before screening. Pts who have demonstrated at least a minimal response to teclistamab (assessed during the 8-week screening period based on International Myeloma Working Group criteria) will be randomized 2:1 to receive IVIG 10% 400 mg/kg every 3–4 weeks as either primary infection (from randomization) or secondary infection (after experiencing ≥1 serious infection) prophylaxis and observed for up to 52 weeks.
The primary endpoint is the time to first serious infection, defined as microbiologically/clinically documented viral/bacterial/fungal infection requiring ongoing treatment with intravenous anti-infectives (confirmed by an independent endpoint adjudication committee). Key secondary endpoints are the occurrence of ≥1 serious infection during the observational period, annualized rate of days on antibiotics for treatment of bacterial infections and annualized rate of bacterial infections. Safety endpoints include the occurrence of adverse events, treatment-emergent adverse events (TEAEs), TEAEs related to IVIG 10% and TEAEs temporally associated with IVIG 10% (within 72 hours). Tolerability assessments include the number of infusion withdrawals/interruptions/rate reductions owing to TEAEs. The impact of IVIG 10% treatment on health care resource utilization will also be evaluated.
Results:
In total, 183 pts are planned for enrollment (122 and 61 in the primary and secondary infection prophylaxis arms, respectively).
Conclusions:
This study will provide critical evidence on the efficacy, safety and tolerability of IVIG 10% as primary infection prophylaxis in pts with MM receiving BCMA×CD3-directed BsAb therapy. These results will support the development of appropriate strategies and guidance for infection prevention in this population who are at high risk of developing severe infections.
Study/writing funder: Takeda Development Center Americas, Inc./Takeda Pharmaceuticals International AG.