
Myeloma Novel Drug Targets and agents
Category: Myeloma Novel Drug Targets and agents
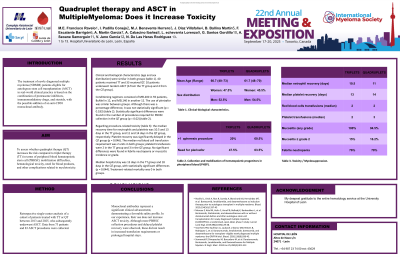
Quadruplet Therapy and ASCT in Multiple Myeloma: Does It Increase Toxicity?
 photo")
Eloy Francisco, EF (he/him/his)
MD
Complejo Asistencial Universitario de León
El tratamiento de los pacientes con mieloma múltiple (NDMM) recién diagnosticados elegibles para trasplante autólogo de células madre (ASCT) en la práctica clínica real se basa en la combinación de inhibidores del proteasoma, fármacos inmunomoduladores y esteroides, con la posible adición de un anticuerpo monoclonal anti-CD38.
Methods:
To assess whether quadruplet therapy (QT) increases the risk compared to triplet therapy (TT) in terms of peripheral blood hematopoietic stem cell (PBHSC) mobilization difficulties, hematological toxicity, need for blood products, and other complications related to myelotoxicity.
Análisis retrospectivo unicéntrico de una cohorte de pacientes tratados con TT o QT entre 2013 y 2025, a los que posteriormente se les realizó un TCMA. Se recogieron datos de 73 pacientes y 83 procedimientos de TCAS.
Results:
Clinical and biological characteristics (age and sex distribution) were similar in both groups. Forty patients received TT and 33 received QT. Ten patients underwent tandem ASCT (6 from the TT group and 4 from the QT group).
Conditioning regimens consisted of MEL200 in 59 patients, BuMel in 12, and MEL140 in another 12. The use of plerixafor was similar between groups. Although there was a percentage difference, it was not statistically significant (p = 0.183). Statistically significant differences were found in the number of procedures required for PBHSC collection in the QT group (p = 0.02).
Regarding procedure-related toxicity: the median recovery time for neutrophils and platelets was 10.5 and 13 days in the TT group, and 11 and 14 days in the QT group, respectively. Platelet recovery was significantly delayed in the QT group (p = 0.046). The median red blood cell transfusion requirement was 2 units in both groups; platelet transfusions were 2 in the TT group and 3 in the QT group. No significant differences were found in febrile neutropenia or mucositis incidence or grade.
La mediana de estancia hospitalaria fue de 15 días en el grupo TT y de 18 días en el grupo QT, con diferencias estadísticamente significativas (p = 0,044). La mortalidad relacionada con el tratamiento fue 0 en ambos grupos.
Conclusions:
Los anticuerpos monoclonales representan un avance clínico significativo, demostrando un perfil de seguridad favorable. En nuestra experiencia, su uso no aumenta la toxicidad de ASCT. Aunque se observaron más procedimientos de recolección de PBHSC, estancias hospitalarias prolongadas y recuperación tardía de plaquetas, estos no resultaron en un aumento de los requisitos de transfusión.