
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
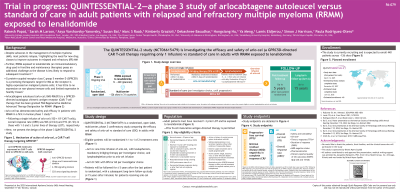
Trial in Progress: QUINTESSENTIAL-2—A Phase 3 Study of Arlocabtagene Autoleucel Vs Standard of Care in Adult Patients With Relapsed and Refractory Multiple Myeloma (RRMM) Refractory to Lenalidomide
.jpg "Rakesh Popat, BSc, MBBS, MRCP, FRCPath, PhD photo")
Rakesh Popat, BSc, MBBS, MRCP, FRCPath, PhD
Consultant Haematologist
NIHR UCLH Clinical Research Facility, University College London Hospitals NHS Foundation Trust, London, UK
Despite advances in MM treatment, nearly all patients (pts) will relapse, highlighting the need for new drug classes to improve outcomes in RRMM. Further, MM refractory to lenalidomide, an immunomodulatory drug (IMiD) used in frontline and maintenance therapies, poses an additional challenge as the disease is less likely to respond to subsequent treatment. G protein-coupled receptor class C group 5 member D (GPRC5D) is a promising therapeutic target for MM as the receptor is highly expressed on malignant plasma cells; it has little to no expression on non-plasma immune cells and limited expression elsewhere. Arlocabtagene autoleucel (arlo-cel) is a GPRC5D-directed autologous CAR T-cell therapy that has demonstrated safety and efficacy in pts with RRMM in a first-in-human phase 1 study. Following a single infusion of arlo-cel (150×106 CAR T-cells), overall response rate (ORR) was 96% (23/24) and 91% (21/23) in those with 1-3 and ≥3 prior lines of therapy (pLOT), respectively (Bal S, et al. ASH 2024. Abstracts 2069 and 922). We present the design of QUINTESSENTIAL-2 (NCT06615479), a randomized, open-label, multicenter, phase 3 confirmatory study comparing the efficacy and safety of arlo-cel versus standard of care (SOC) in adults with RRMM.
Methods:
Pts aged ≥18 y must have received 1-3 pLOT (may include a proteasome inhibitor, IMiD, and anti-CD38 antibody), be refractory to lenalidomide (progression on or within 60 days of completing therapy), and have confirmed MM diagnosis per International Myeloma Working Group criteria, measurable disease during screening, and ECOG performance status 0 or 1. Eligible pts will be randomized 1:1 to Arm-A or Arm-B. Pts randomized to Arm-A will receive a single infusion of arlo-cel, including leukapheresis within 3 days of randomization, bridging therapy of DPd (daratumumab, pomalidomide, dexamethasone) or Kd (carfilzomib, dexamethasone) per Investigator choice within 3 days of leukapheresis, and lymphodepleting chemotherapy prior to arlo-cel infusion. Pts randomized to Arm-B will receive SOC of DPd or Kd per Investigator choice, dosed per labeling. Primary endpoints are progression-free survival and minimal residual disease (MRD) negativity in complete response. Secondary endpoints include overall survival, ORR, MRD-negative status, complete response rate, time to response, duration of response, pharmacokinetics, patient-reported quality of life outcomes, and safety. Pts will be followed for ≤5 years after the last pt is randomized, with a subsequent long-term follow-up study (≤15 years post-infusion) for pts receiving arlo-cel.
Results:
This is a trial in progress and is expected to enroll 440 pts at over 100 sites globally. The first pt was enrolled in March 2025.
Conclusions: This phase 3 study will compare the efficacy and safety of arlo-cel versus SOC in adult pts with RRMM who are refractory to lenalidomide.