
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
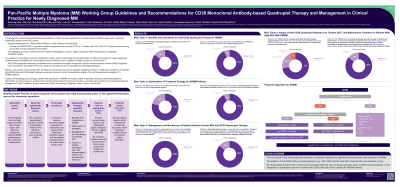
Pan-Pacific Multiple Myeloma (MM) Working Group Guidelines and Recommendations for CD38 Monoclonal Antibody-based Quadruplet Therapy and Management in Clinical Practice for Newly Diagnosed MM

Wenming Chen
Chief Physician
Department of Hematology, Beijing Chaoyang Hospital, Capital Medical University
Incorporating anti-CD38 monoclonal antibodies (mAbs), including isatuximab and daratumumab, into the bortezomib/lenalidomide/dexamethasone (VRd) therapy backbone as first-line (1L) treatment for newly diagnosed MM (NDMM) has demonstrated improved efficacies and no additional safety concerns. Based on these results, the National Comprehensive Cancer Network Guidelines Version 1.2025 was updated to incorporate anti-CD38 mAbs with VRd-based therapies as primary therapy for both transplantation-eligible (Te) and transplantation-ineligible (Ti) NDMM patients (pts). A panel of hematology and oncology experts with experience in NDMM convened in 2024 to develop consensus recommendations based on evidence from pivotal clinical trials and real-world practices, providing clear guidance for optimizing treatment strategies in Te and Ti pts.
Methods:
A modified Delphi consensus process was employed to generate statements regarding the use of anti-CD38 mAb quadruplet (quad) therapy in NDMM, using anonymous online voting and in-person meetings. A steering committee formulated 8 statements for online voting and a meeting was held to discuss and finalize the statements. The main topics identified for discussion for quad therapy in NDMM were: benefits and indications; optimization strategies; management and monitoring of potential adverse events (AEs), and the impact on tandem stem cell transplantation and maintenance treatment.
Results:
Of 14 voters, 85.7% agreed that anti-CD38-based quad therapy is suitable for Ti NDMM pts and 92.9% agreed it was suitable as 1L treatment for Te pts. Quad therapy is preferred for pts < 80 years old who are not frail (78.6% consensus) and for those with mild renal impairment (92.9% consensus). All voters agree that hematologic toxicities are among the most common AEs in pts undergoing quad therapy, and management supports are recommended. There was 85.7% agreement that quad regimens may increase infection susceptibility; therefore, prophylactic antiviral and antibacterial agents and vaccinations are advised prior to initiating therapy. For high-risk pts receiving tandem autologous stem cell transplant (ASCT), 71.4% agreed that stem cell collection should be planned before the fourth cycle. Following induction and ASCT, 85.7% agreed that lenalidomide remains the cornerstone of maintenance therapy and a more aggressive strategy may be considered in pts with high-risk cytogenetic abnormalities or those who achieved minimal residual disease negativity.
Conclusions:
The use of anti-CD38 mAb quad therapies represents a significant advancement in the treatment of NDMM. The addition of anti-CD38 mAbs to VRd-based regimens has the potential to become the new standard of care. By incorporating evidence from clinical trials and expert opinions, this consensus provided clear, evidence-based guidance on the integration of quad regimens into clinical practice for NDMM, particularly for Ti pts.
Funding: Sanofi. Recently published: Chen W, et al. Clin Hematol Int 2025;7(2):1-19.