
Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
Category: Treatment of Newly Diagnosed Myeloma (excluding t-cell redirection therapy)
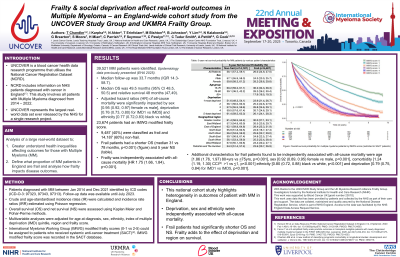
Frailty and social deprivation affect real-world outcomes in Multiple Myeloma (MM) – an England-wide cohort study from the UNCOVER Study Group and UKMRA Frailty Group.

Thea Chandler, MBChB BSc MRCP
Haematology Registrar
Leeds Teaching Hospitals Trust
39,521 MM patients were identified in total. Crude and age-standardised IR were higher for older people, males and black people. Crude but not age-standardised IR were lower for more deprived areas. Adjusted IRRs increased with age and were lower for females [0.62 (p< 0.001)], less deprived areas [0.95 (p=0.006) for IMD5 vs 1), and all provincial regions vs London [e.g. 0.63 (p< 0.001) for North West]. Median follow-up was 33.7 (IQR: 14.3–58.7) months. 21,987 (55.6%) patients died with median OS 49.5 (48.5–50.5) months and NS
58.7% and 45.3% at 3 and 5 years. Hazard of all-cause mortality was higher for males [1.06 (1.03–1.08)] and increased with age [10.2 (8.1–12.1) for 81–99 compared to < 40], deprivation [1.29 (1.22–1.34) for IMD1 vs 5], comorbidity [1.46 (1.41–1.50) for CCI >1 vs ≤1], and provincial regions vs London [1.21 (1.15–1.28) for North West].
Among the 23,674 (60%) patients with an IMWG frailty score, 9,487 (40%) were classed as frail and 14,187 (60%) non-frail. Frail patients had a shorter OS (median 31 vs 78 months, p< 0.001) and NS (58.1% vs 73.1% at 3 years; 26.0% vs 44.5% at 5 years). This extended to high-risk subgroups defined by deprivation or region (5-year NS: 23.9% vs 51.6% for IMD1; 22.6% vs 55.9% for North East). Frailty was independently associated with all-cause mortality (HR 1.75, p< 0.001).