
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
Real-world Outcomes Among Patients (Pts) with Relapsed or Refractory Multiple Myeloma (RRMM) Initiating Teclistamab (Tec) at a Large Community Oncology Center in the US
Yair Levy, MD
Director of Hematologic Malignancies Research
Texas Oncology, Dallas, TX, USA
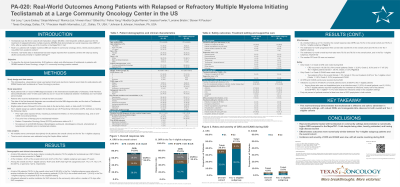
Patient chart and EMR data for adult pts with RRMM and ≥1 record for Tec between 10/26/2022 - 12/31/2024 were used. Pts were followed from index (date of first Tec SUD) to the earliest of last activity, death, or data cutoff. All variables were summarized descriptively for all pts (overall) and for subgroup of pts who would have been MajesTec-1 eligible (Tec-eligible). Time-to-event outcomes were estimated using the Kaplan-Meier method.
Results:
A total of 50 pts met the study criteria (median [IQR] age 73 years [45-88]; 70% White; 18% Black; 36% R-ISS stage III; 46% high-risk cytogenetics; 6% ECOG ≥2; 6% prior BCMA exposure). Of the 50 pts, 37 (74%) were Tec-eligible (median age [IQR], 73 years [45-88]; 84% White; 14% Black; 32% R-ISS stage III; 43% high-risk cytogenetics). Both cohorts had a median of 4 prior lines of therapy. A total of 38 pts (76%) in overall and 30 (81%) in Tec-eligible were referred to another institution for inpatient SUD, while the remaining pts (12 [24%] in overall and 7 [19%] in Tec-eligible) completed SUD in the outpatient setting. All pts referred to another institution for SUD returned to the community clinic for first treatment dose within a median of 15 days after SUD completion. During SUD, cytokine release syndrome (CRS) occurred in 19 (38%) overall pts (32% Grade [G]1, 6% G2) and 17 (46%) Tec-eligible pts (38% G1, 8% G2); 2 pts in both cohorts experienced immune effector cell-associated neurotoxicity syndrome (ICANS; 1 G1, 1 G2). All CRS and ICANS events were resolved. At a median follow-up of 14.3 months, infections occurred in 34 (68%) overall pts and 27 (73%) Tec-eligible pts; only 4 needed hospitalization for treatment of infections, while others were resolved outpatient. Pts received a combination of antibiotics, antivirals, IVIG as prophylaxis for infections; 46% pts received at least one dose of IVIG prophylaxis in both cohorts. The overall response rate was 74% in all pts and 73% in Tec-eligible. Estimated 12-month PFS rate was 65% in overall and 76% in Tec-eligible pts; 12-month OS rates were 75% and 78%, respectively.
Conclusions:
Overall, pts treated with Tec in community settings experienced numerically comparable effectiveness and safety outcomes as compared with MajesTec-1 trial, despite being elderly with high-risk cytogenetics, high disease burden, and heavily pretreated pts. Most adverse events were low grade, highlighting the feasibility of safely administering Tec and effectively managing AEs in outpatient and/or community settings.