
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
Bispecific Outpatient Step-Up Dosing with Prophylactic Dexamethasone: The BOSS Program Experience in Myeloma

Diana Cirstea, MD
Medical Oncologist
Center for Multiple Myeloma, Massachusetts General Hospital, Harvard Medical School
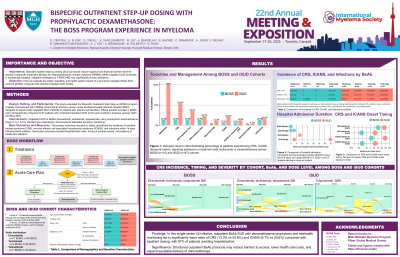
While outpatient step-up dosing (SUD) for bispecific antibodies (BsAbs) is increasingly adopted, mitigation strategies for CRS/ICANS vary significantly across institutions. The BOSS (Bispecific Outpatient Safe Step-up) program at MGH implements a distinctive approach using prophylactic dexamethasone without preemptive tocilizumab, combined with structured remote monitoring.
The BOSS program was designed to facilitate outpatient administration of BsAbs for patients with plasma cell disorders, allowing SUD on Days 1 and 3, followed by full dose on Day 8. Supportive care included standard pre-medications on BsAb days plus prophylactic dexamethasone (12 mg on Days 2, 4-7, and 9-10) and daily telehealth symptom assessments. A retrospective analysis was conducted on 15 patients enrolled in the BOSS program (elranatamab n=11, teclistamab n=3, talquetamab n=1), who met eligibility criteria (adequate organ function, low disease burden, and proximity to the treatment facility). Additionally, data were collected from 97 patients who received standard inpatient SUD (iSUD), focusing on CRS, ICANS, and infection rates through Day 14.
A total of 112 patients who received all SUD and first full dose were included (median age 72 years). The BOSS cohort (n=15) had 13.3% CRS (2/15, 0% recurrent, all G2 with median onset 41 hours post-SUD#1), 6.7% ICANS (1/15, G1), 13.3% infections (2/15), and 87% with no hospital stay (13/15). The iSUD cohort (n=97) had 53.6% CRS (52/97, 11% recurrent, 41% max G1, 12% max G2), 20.6% ICANS (20/97, G1-3) and 16.5% infections (16/97), with a median 8-day hospital stay. The timing of CRS differed; CRS in BOSS occurred exclusively post-SUD#1, vs. CRS in iSUD were 34% post-SUD#1, 42% post-SUD#2, 11% post-SUD#3 (talq q2w only) and 13% post-full dose. The median onset for ICANS occurred earlier in BOSS (6 hours) compared to iSUD (77 hours). Table 1 presents the incidence of CRS, ICANS, and infections classified by each BsAb for both BOSS and iSUD cohorts.
Table 1: Incidence of CRS, ICANS, and Infections by BsAb in BOSS and iSUD Cohorts
| BOSS | iSUD | ||||||
Elran n=11 | Tec n=3 | Talq n=1 | Total n=15 | Elran n=30 | Tec n=28 | Talq n=39 | Total n=97 | |
CRS, n (%) | 2 (18.2%) | 0 | 0 | 2 (13.3%) | 16 (53.3%) | 13 (46.4%) | 23 (59.0%) | 52 (53.6%) |
ICANS, n (%) | 1 (9.1%) | 0 | 0 | 1 (6.7%) | 7 (23.3%) | 6 (21.4%) | 7 (17.9%) | 20 (20.6%) |
Infections, n (%) | 1 (9.1%) | 1 (33.3%) | 0 | 2 (13.3%) | 6 (20%) | 3 (10.7%) | 7 (17.9%) | 16 (16.5%) |
The BOSS program’s outpatient SUD strategy, featuring prophylactic dexamethasone without preemptive tocilizumab, led to markedly lower rates of CRS (13 vs. 54%) and ICANS (7% vs. 21%) compared to historical inpatient management. With 87% of patients avoiding hospitalization, this approach offers a viable alternative for select myeloma patients receiving BsAbs. Outcomes analysis is in progress to further assess the long-term implications of BOSS strategy. These results support further evaluation of optimized outpatient protocols to improve patient convenience and resource utilization.