
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
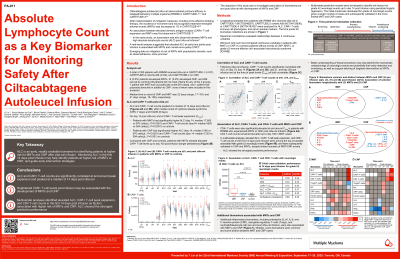
Absolute Lymphocyte Count as a Key Biomarker for Monitoring Safety After Ciltacabtagene Autoleucel

Yi Lin, MD, PhD
Professor of Medicine
Mayo Clinic
Ciltacabtagene autoleucel (cilta-cel) demonstrated high efficacy in relapsed/refractory multiple myeloma (RRMM) in CARTITUDE-1 and CARTITUDE-4. After implementation of mitigation measures, the incidence of movement and neurocognitive treatment-emergent adverse events (MNT) decreased to 1% in CARTITUDE-4. An association between elevated CAR+ T-cell expansion and MNT was first seen in CARTITUDE-1 (Cohen, et al. Blood Cancer J 2022). A real-world analysis suggested that elevated absolute lymphocyte count (ALC) at early time points post infusion was associated with MNT and cranial nerve palsy (CNP) (Lim, et al. TANDEM 2025, p274). Herein, we investigated biomarkers associated with MNT/CNP pre and post cilta-cel.
Methods: Longitudinal samples from patients (pts) with RRMM who received cilta-cel in CARTITUDE-1 (n=97), CARTITUDE-2 cohorts A/B (n=62), and CARTITUDE-4 (n=196) were analyzed for ALC, immune cell phenotypes, and serum soluble markers. Spearman correlations evaluated relationships between 2 continuous variables. Wilcoxon rank sum test compared continuous variables in pts with MNT/CNP vs controls (pts without CNP, MNT, or grade ≥2 immune effector cell–associated neurotoxicity syndrome [ICANS]). Logistic regression models were fit to predict MNT/CNP and to identify multivariable associations.
Results: ALC and CAR+ T-cell counts peaked at a median of 14 days (d) post cilta-cel, after the median onset of cytokine release syndrome (7d) and ICANS (8d). ALC and CAR+ T-cell counts correlated significantly d10-28 post infusion and at peak expansion (d14: R=0.79; P< 0.0001). Eight (2.3%) pts developed MNT and 20 (5.6%) CNP; 288 served as controls (39 did not meet criteria). Median time to CNP and MNT onset was 22d and 41d, respectively. Pts with MNT had significantly higher CAR+ T-cell counts (median 5520 vs 384 cells/µL; P< 0.0001) and ALC (median 17,600 vs 970 cells/µL; P< 0.0001) vs controls on d14 post cilta-cel. Pts with CNP also had significantly higher CAR+ T-cell counts (median 1230 vs 384 cells/µL; P< 0.001) and ALC (median 2180 vs 970 cells/µL; P< 0.0001) vs controls on d14. Despite limited numbers of MNT/CNP events, multivariate analyses identified elevated ALC, CAR+ T-cell peak expansion, and CD4+ T-cell counts in the first 14d post infusion as biomarkers associated with MNT/CNP, with ALC showing the strongest association. Additional inflammatory biomarkers, including IL-6, IL-8, C-reactive protein, alongside regulatory T cells, and neutrophil/leukocyte ratio pre and post cilta-cel infusion, were also associated with MNT/CNP.
Conclusions: These data suggest that heightened CAR+ T-cell expansion levels post infusion may be associated with MNT/CNP. ALC is an early biomarker for identifying pts at risk for MNT/CNP after cilta-cel infusion, at and closely before/after peak CAR+ T-cell expansion, which may help guide closer monitoring and preemptive interventions (eg, short course dexamethasone [Turner, et al. TANDEM 2025, p290]).