
Plasma Cell precursor and Other Disorders
Category: Plasma Cell precursor and Other Disorders
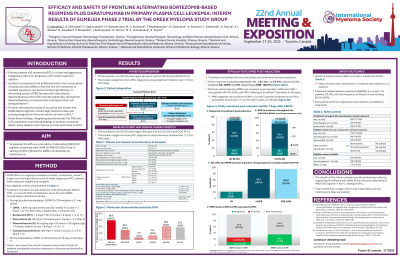
EFFICACY AND SAFETY OF FRONTLINE ALTERNATING BORTEZOMIB-BASED REGIMENS PLUS DARATUMUMAB IN PRIMARY PLASMA CELL LEUKEMIA: INTERIM RESULTS OF EUMELEIA PHASE 2 TRIAL BY THE GREEK MYELOMA STUDY GROUP.
 photo")
Eirini Katodritou, MD (she/her/hers)
Hematologist, Director, Head of the Department of Hematology
Department of Hematology, Theagenion Cancer Hospital, Thessaloniki, Greece
Primary plasma cell leukemia (pPCL) is a rare and aggressive malignancy with poor prognosis. A phase 2 trial has demonstrated high efficacy of alternating cycles of PAD (bortezomib, doxorubicin, dexamethasone) and CVD (cyclophosphamide, bortezomib, dexamethasone), combined with autologous stem cell transplantation. Our recent retrospective study demonstrated that daratumumab (DARA)-based regimens induce high response rates and prolong survival parameters in pPCL. Given these findings, we evaluated the efficacy and safety of alternating PAD/CVD regimen combined with DARA (D-PAD/D-CVD) in the 1L setting of pPCL followed by DARA monotherapy as maintenance.
Methods:
This is an ongoing investigator-initiated, multicenter, phase 2, single-arm trial aiming to enroll 43 newly diagnosed transplant-eligible or ineligible pPCL patients (pts). Treatment includes a 6-cycle induction with alternating D-PAD/D-CVD, a 2-cycle D-CVD consolidation, and a 24-cycle DARA monotherapy maintenance phase. D-PAD/D-CVD are given in 21-day cycles during induction/consolidation [DARA: 1,800 mg subcutaneously (SC) weekly in Cycle 1-3 (Days 1, 8, 15), then every 3 weeks (Day 1); P/V: 1.3 mg/m2 SC on days 1, 4, 8, 11; A: 30 mg/m2 intravenously on day 4; D: 40 or 20 mg/day orally on days 1, 4, 8, 11; C: 300 mg/m2 orally on days 1, 8], and DARA is administered in 28- day cycles (Day 1) during maintenance. Key inclusion criteria are newly diagnosed pPCL according to the revised International Myeloma Working Group (IMWG) diagnostic criteria of pPCL [≥5% and/or absolute count ≥0.5 × 103/μL circulating plasma cells in peripheral blood (PB) smear or using next generation flowcytometry], age: 18-80, measurable disease, performance status ≤3, adequate bone marrow (BM)/renal/liver function. Main exclusion criteria are severe cardiac/pulmonary dysfunction. This is an interim analysis of the first 20 patients who completed induction or discontinued before this timepoint.
Results:
Between Nov 2021 and Dec 2023, 20 pts (10 pts ≥65 years) were enrolled across six Greek centers. Median time from diagnosis to treatment initiation was 11.5 days (range: 3-44); 19 pts completed the 6-cycle induction phase and were evaluated within 7 days post-induction. Among 19 response-evaluable patients, the overall response rate was 100%, including complete response (21.1%), very good partial response (73.7%) and partial response (5.3%); MRD negativity was achieved in BM in 2 of the 5 pts assessed and in PB in all pts examined (7/7), as for now. Eleven pts were transplant eligible. Grade ≥3 adverse events occurred in 9 pts (45.0%), mainly cytopenias (7 pts) and infections (4 pts). One patient died 30 days post-baseline from respiratory tract infection (unrelated to treatment).
Conclusions:
In conclusion, these results provide preliminary evidence supporting the efficacy and safety of the induction alternating D-PAD/CVD regimen in the 1L setting of pPCL. Final results from a larger cohort with longer follow-up and maintenance data are awaited.