
Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
Category: Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
 photo")
Vania Hungria, MD, PhD (she/her/hers)
Professor
Clinica São Germano
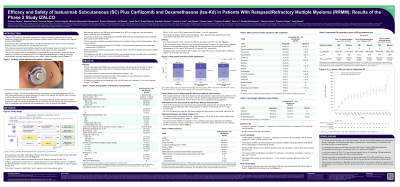
Overall, 74 RRMM pts were enrolled: 8 in Part 1 and 66 in the randomized cohort (Part 2). At study entry, pts had a median age of 65 (44–85) yrs and a median of 1 prior therapy line (1–5); 56.8%, 32.4% and 10.8% had ISS stage I, II or III, respectively. The ORR rate was 79.7% at a median follow-up of 10.1 months, with very good partial response or better in 62.2% of pts and complete response or better in 21.6%. After treatment with both modalities for Isa SC delivery, 74.5% of pts expressed a preference for the OBDS rather than manual injection (p=0.0004); 8.5% had no preference. Grade (G) ≥3 treatment-emergent adverse events (TEAEs) occurred in 54.1% of pts (treatment-related ≥G3 TEAEs in 35.1%) and serious TEAEs in 40.5%. Treatment with Isa SC plus Kd was well tolerated. A single infusion reaction event (1 of G1, 1 of G2) occurred in 2 pts (2.7%, both with manual injection at first dose). Six (8.1%) pts had 18 injection site reactions (17 of G1, 1 of G2) in 1297 (1.1%) manual or OBDS injections. Comparable PK exposure was observed between OBDS and manual administration.
Conclusions:
The study met its primary endpoint, demonstrating efficacy, safety, and similar PK exposure of Isa SC administration in combination with Kd, either by manual injection or OBDS. Our study findings are consistent with those reported in the Phase 3 study IKEMA with intravenous Isa. Pts expressed a clear preference for receiving Isa SC by an OBDS.
Funding: Sanofi. © 2025 American Society of Clinical Oncology (ASCO), Inc. Reused with permission. This abstract was accepted and previously presented at the 2025 ASCO Meeting. All rights reserved.