
Myeloma Genomics and Microenvironment and immune profiling
Category: Myeloma Genomics and Microenvironment and immune profiling
Single cell RNA and whole genome sequencing analysis reveal distinct immune and genomic signatures in WM patients resistant to ibrutinib therapy
 photo")
Tina Bagratuni (she/her/hers)
Senior Researcher
National and Kapodistrian University of Athens
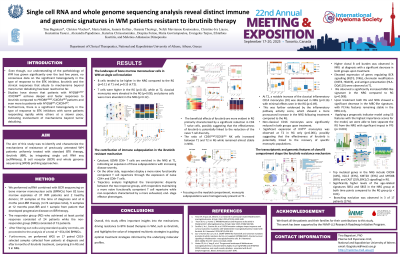
Even though our understanding of the pathobiology of Waldenström’s macroglobulinemia (WM) has grown significantly over the last few years, there is limited data on the heterogeneity that is observed in terms of the depth of response to ibrutinib therapy in clinical responses that allude to mechanisms beyond mere tumor debulking and mechanisms of resistance and treatment failure.
The aim of this study was to identify and characterize the mechanisms of resistance of previously untreated WM patients uniformly treated with standard BTK therapy, ibrutinib (IBR), by integrating single cell RNA seq (scRNAseq), B cell receptor (BCR) and whole genome sequencing (WGS) profiling approaches.
Methods:
We performed scRNA combined with BCR sequencing on bone marrow mononuclear cells (BMNCs) from 62 bone marrow aspirates of 27 WM patients and 2 healthy donors; 27 samples at the time of diagnosis and at 6 moths post-IBR therapy (n=54 samples total), 3 samples at 12 months post-IBR and 3 samples from patients that developed progressive disease on ΙBR therapy. The responder group (RG) who achieved at least partial response consisted of 17 patients while the non-responder group (NRG) consisted of 10 patients. After filtering out cells using standard quality controls, we proceeded to the analysis of a total of ~260,000 BMNCs.
Results:
Our results showed significantly more clonal B cell population in the NRG at diagnosis compared to the RG (p=0.03) and identified genes such as CHST15, EIF4E3, GSDME, IL17RB upregulated in RG and genes such as EGR1, S100A4, S100A6 upregulated in NRG. Regarding the immune microenvironment, IFN+ monocytes in NRG were significantly increased compared to the RG (p= 0.005) at diagnosis, and SELL+ NK subpopulation was more prominent. CD4 and CD8 T naive cells were significantly enriched in the RG while subpopulations exhibiting more exhausted phenotype, such as the GZMB+, were more common in the NRG. We also observed significant increases of the GZMK+ T cell effector subpopulation post-IBR in NRG (p= 0.005) while a significant decrease of the naïve CD8 T cells and Tregs was observed post-IBR in the RG only.
Mutational analysis identified highly mutated genes in the RG including KMT2C (25%), CAST (25%), and SLC10A3 (25%) while in the NRG included CXCR4 (44%), NOTCH1 (33%), KMT2D (33%), ARID1A (22%) and ARID1B (22%). Amplifications of chromosomes 12 (40% in NR group) and 18 (25% in NR group) were only seen in the NRG while del6q was observed in about 40% of the NRG compared to 25% in the RG.
Conclusions:
In conclusion, our results show distinct transcriptomic, genomic and immune profiles between WM patients with different responses to ibrutinib therapy, highlighting potential mechanisms of resistance that could serve for the identification of predictive biomarkers for BTK-based therapy in WM.