
Cellular and T cell engager Immunotherapy
Category: Cellular and T cell engager Immunotherapy
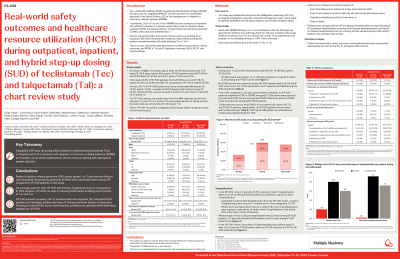
Real-world safety outcomes and healthcare resource utilization (HCRU) during outpatient, inpatient, and hybrid step-up dosing (SUD) of teclistamab (Tec) and talquetamab (Tal): a chart review study
.jpg "Cindy Varga, MD photo")
Cindy Varga, MD
Associate Professor
Levine Cancer institute/Atrium Health
Traditionally, SUD of Tec and Tal for relapsed/refractory multiple myeloma (RRMM) has been conducted in inpatient (IP) settings to manage cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). SUD is increasingly administered outpatient (OP) to expand patient (pt) access and reduce HCRU. This real-world study describes the safety outcomes and hospitalizations of Tec or Tal pts receiving SUD in OP, IP, and hybrid (mixed OP/IP) settings.
Methods:
This study used data from a medical record review of RRMM pts receiving Tec or Tal post-FDA approval across a consortium of US sites. Pts were categorized by intended SUD setting: OP, IP, or hybrid. Pt characteristics, safety outcomes, and hospitalizations were described for each cohort.
Results:
The OP, IP, and hybrid cohorts had 21 (Tec: 17; Tal: 4), 132 (Tec: 93; Tal: 39), and 68 (Tec: 36; Tal: 32) pts, respectively. Median age at treatment initiation for OP pts was 75.0 years (IP: 68.8 years; hybrid: 66.5 years); OP pts were 66.7% White and 28.6% Black (IP: 82.6% and 14.4%; hybrid: 75.0% and 16.2%). Of OP pts, 23.8% had ECOG score ≥2 (IP: 38.6%; hybrid: 26.4%) and 28.6% had high-risk cytogenetics (IP: 54.5%; hybrid: 55.9%). The OP cohort received a median of 4 prior lines of treatment (IP: 6; hybrid: 5).
All but 1 IP pt completed all SUD doses. During SUD, 33.3% of OP pts had CRS (IP: 59.8%; hybrid: 55.9%), with no grade 3+ events for OP and hybrid pts and only 4 (3.0%) IP pts reaching grade 3. ICANS occurred in 11.4% of the IP cohort and 7.4% of the hybrid cohort, with no events among OP pts. From SUD completion to 30 days post-treatment initiation, no OP pts experienced CRS or ICANS, but 1 additional grade 2 CRS event was reported in IP and hybrid cohorts each as well as 1 ICANS event in the hybrid cohort.
In IP and hybrid cohorts, 47.7% and 30.9% of pts received tocilizumab to treat CRS, respectively; no OP pt was treated with tocilizumab. Two-thirds (66.7%) of OP pts received steroids during SUD (IP: 47.7%; hybrid: 73.5%) with 14.3% for CRS management (IP: 15.9%; hybrid: 19.1%), and 4.8% for other neurotoxicity event management (IP: 7.6%; hybrid: 4.4%).
In the OP cohort, 2 pts (9.5%) required hospitalization. Median length of stay (LOS) per hospitalization was shortest among OP pts (2 days), followed by hybrid (2.3 days) and IP pts (8 days). The number of days hospitalized per pt was 0.2 days per OP pt vs 9.2 days per IP pt which is a 97.9% reduction in LOS for OP pts.
Conclusions:
In this real-world study of Tec and Tal pts, while OP pts were older than IP and hybrid pts, they had lower risk disease. These differing pt profiles and numerically lower rates of CRS and ICANS among OP pts (CRS mainly grade 1/2) highlight the importance of appropriate pt selection for OP SUD. SUD initiation in OP settings reduced HCRU compared to hybrid or IP. These findings demonstrate OP and hybrid SUD models are feasible, can be safely implemented, and resource‐sparing with appropriate pt selection.