
Nursing and Allied Health Symposium
Category: Nursing & Allied Health Symposium
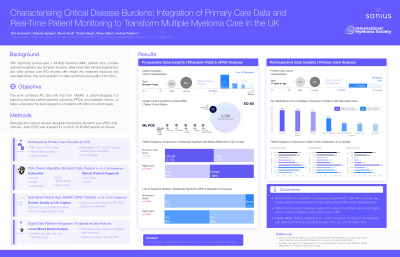
Characterising Critical Disease Burdens: Integration of Primary Care Data and Real-Time Patient Monitoring to Transform Multiple Myeloma Care in the UK
 photo")
Hannah L. Miller, MPharm (she/her/hers)
Lead Macmillan Pharmacist
The Christie NHS Foundation Trust
With improving survival rates in Multiple Myeloma (MM), patients face complex treatment regimens and symptom burdens. Real-world data remains fragmented, and while primary care (PC) records offer insight into treatment exposure and care trajectories, they lack resolution on daily symptoms and quality of life (QoL). This work combined PC data with that from ‘MyMM’, a patient-designed tool capturing real-time patient-reported outcomes (PROs) and wearable metrics, to better understand MM burden and unmet needs.
Methods:
Retrospective analysis was performed for 275 UK patients with MM-linked CTV3 codes in PC records, linked across events, medications, and demographics. Prospective data (n=36) from MyMM’s PRO interface (e.g., EQ-5D-5L and symptoms extracted from ‘My POS’) alongside wearable (n=19) metrics through an FDA-approved device were collected (Jan-May 2025). Variation by sex, age, and treatment line was analysed for all metrics using a linear mixed model.
Results:
The PC cohort (51% female; mean age 77 (53–99)) had a mean of 11 years since first recorded diagnosis; 186 were deceased at censure (53%; 79 (53–99)). Patients had a mean of 20 unique repeat PC-issued medications (excluding hospital prescriptions, most commonly Lansoprazole (44%), Paracetamol (43%), and Amlodipine (41%)) and 31 CTV3 codes (essential hypertension (27%), deep venous thrombosis (17%), lower back pain (16%), and type II diabetes (15%)) over their PC history, with 16 clinical PC contacts annually post-diagnosis.
Females had higher prescribing (21.5 vs. 18.4) and comorbidity burden (35.5 vs. 25.5) than males. Patients aged 80+ had fewer contacts but greater comorbidity (34.5) and prescribing (22.5). Annual events and repeat prescriptions increased stepwise with rising code counts and assumed complexity.
App data (58% female; age 58 (36-78)) over a median 70 (7-126) days captured 38,827 datapoints: 4,561 activity, 4,207 sleep, and 30,023 PRO. 23 patients reported first (1L), 4 second (2L), 3 third-line or above (3L+), and 4 off treatment.
Weakness demonstrated the highest severity score (1=least-5=most) at 3.8, followed by drowsiness (2.7), poor mobility (2.6), tingling (2.5), and difficulty remembering (2.0). EQ-5D-5L averaged 0.706 and VAS 66.0.
Borderline significant sex-based differences were seen in EQ-5D-5L (female: 0.703 vs. male: 0.575, p=0.051), with significant differences in nightly SpO2 (96% vs. 98%, p=0.002). Tingling severity increased with age (+0.085/year, p=0.031). 3L+ patients showed higher ‘shortness of breath’ than off treatment (4.9 vs. 0.5, p=0.050), and 1L recorded higher nightly SpO2 than 3L+ (98% vs. 96%, p=0.046).
Conclusions:
This work demonstrates the feasibility of integrating longitudinal PC data with real-time app-based symptom and biometric monitoring to deepen MM burden characterisation. Differences by patient subgroup were evident across both datasets, with findings supporting the value of combined clinical and digital data to enhance stratified, personalised care in MM.