
Plasma Cell precursor and Other Disorders
Category: Plasma Cell precursor and Other Disorders
Integrative Clinical, Transcriptomic, and Immunohistochemical Characterization of Light Chain Amyloidosis in Bone Marrow and Cardiac Tissue

Chao-Hung Wei, MD
Physician
National Taiwan University Cancer Center
Systemic light chain (AL) amyloidosis is a rare and potentially fatal plasma cell dyscrasia in which misfolded immunoglobulin light chains form amyloid fibrils that deposit in organs and cause irreversible damage. While the clinical manifestations are heterogeneous and often overlap with other plasma cell disorders such as multiple myeloma (MM) and monoclonal gammopathy of undetermined significance (MGUS), the underlying immune and transcriptomic features of AL amyloidosis remain insufficiently characterized.
Methods:
We retrospectively reviewed 50 patients with newly diagnosed primary AL amyloidosis treated at a tertiary medical center in Taiwan. Clinical characteristics, treatment responses, and survival outcomes were analyzed. PD-1 immunohistochemical (IHC) staining was performed on bone marrow and cardiac biopsy tissues. Bulk RNA sequencing was conducted on cryopreserved bone marrow specimens from AL amyloidosis (n=12), MM with coexisting amyloidosis (n=5), and MGUS (n=15) cohorts. Differentially expressed genes (DEGs) were identified using DESeq2, followed by Gene Ontology (GO) and KEGG enrichment analyses. A subset of immune-related DEGs was analyzed separately.
Results:
Cardiac involvement was observed in 80% and renal involvement in 64% of patients. Mayo 2012 staging stratified overall survival (OS) effectively, while renal staging was predictive of dialysis risk. The 3-year OS rate was estimated at 73.97%. Treatment modality significantly impacted prognosis, with better OS seen in patients receiving bortezomib- or alkylating agent-based therapies.
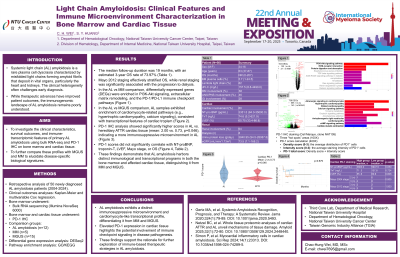
In transcriptomic analysis, AL amyloidosis and MM demonstrated distinct expression profiles. A total of 153 DEGs were identified, including upregulation of mitochondrial and immune-regulatory genes in AL. Enrichment analyses revealed pathways related to extracellular matrix remodeling, PI3K-Akt signaling, and PD-1/PD-L1 immune checkpoint regulation. PD-1 IHC staining confirmed higher scores in AL cardiac tissues compared to hereditary cardiac ATTR amyloidosis (mean: 2.00 vs. 0.73, p = 0.046), though PD-1 levels did not correlate with NT-proBNP or OS.
Comparison between AL amyloidosis and MGUS identified 738 DEGs, with 595 genes upregulated in AL. These included genes involved in mitochondrial respiration and cardiomyocyte function (e.g., ATP6, ND4, COX1), whereas MGUS samples exhibited higher expression of ribosomal and immune-related genes. GO and KEGG analyses revealed enrichment in muscle differentiation, calcium signaling, and cardiomyopathy-related pathways in AL, aligning with the disease’s known cardiac tropism.
Conclusions: This integrative analysis highlights the clinical heterogeneity and immunogenomic complexity of AL amyloidosis. PD-1 pathway activation and cardiac-specific transcriptomic signatures may underlie the disease’s immune suppression and tissue tropism. These findings offer new insights into AL pathophysiology and support further exploration of immune-targeted therapies.