
Myeloma Genomics and Microenvironment and immune profiling
Category: Myeloma Genomics and Microenvironment and immune profiling
Treatment of Plasma Cell Disorders Post Solid Organ Transplant – A Positive Single Center Experience using Immunomodulatory Drugs
 photo")
Khalida B. Soki, MD (she/her/hers)
Transplant Nephrology Fellow
University of Alberta
We conducted a retrospective chart review of all SOT recipients at our center, from 2016 to 2025, who were treated for plasma cell disorders. Data collected included transplant type, treatment details & patient & allograft outcomes.
Results:
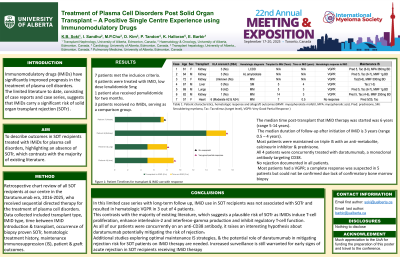
7 patients met the inclusion criteria: 4 received IMiD, lenalidomide 5mg, 1 patient also received pomalidomide & 3 patients received no IMiDs, serving as a comparison group. Clinical indications for IMiD included treatment of de novo disease, relapsed disease & maintenance therapy. Median time post-transplant to IMiD therapy initiation was 6 years (range 5-14 years). Median duration of follow-up after initiation of IMiD was 3 years (range 0.5–4 years). Most patients were maintained on triple IS. Of note, all 4 patients were concurrently treated with daratumumab, a monoclonal antibody targeting CD38. There was no rejection documented in all patients.
Case | Age | Sex | HLA Mismatch (DSA) | Haematological Diagnosis | Transplant to IMiD (Years) | Time on IMiD (Years) | Haematological response to IMiD | IS |
1 | 61 | F | 3 | LCDD | - | - | VGPR | Pred 5, Tac (6-8), MPA 360mg BD |
2 | 64 | M | 3 | AL Amyloidosis | - | - | VGPR | Pred 5, Tac (6-7), MMF 1g BD |
3 | 72 | F | Unknown | MM | - | - | VGPR | Tac (5-6), MMF 500mg BD |
4 | 67 | M | 0 | SM | 5 | 4 | VGPR | Tac (1-3) |
5 | 69 | M | 6 (A2) | MM | 5 | 3 | VGPR | Pred 5, Tac (6-7), MMF 1g BD |
6 | 82 | M | 1 | MM | 15 | 3 | VGPR | Pred 5, Tac (4-6), MMF 250mg BD |
7 | 57 | F | 6 (Moderate A2, A24) | MM | 7 | 0.5 | No response | Pred 5/25, Tac |
Table 1: Patient characteristics, hematologic response & allograft outcomes (MMF: mycophenolate mofetil, MPA: mycophenolic acid, Pred: prednisone, SM: Smouldering myeloma, Tac: Tacrolimus (target level), VGPR: Very Good Partial Response)
Conclusions:
In this case series, IMiD use in SOT recipients was not associated with SOTr & resulted in hematologic VGPR in 3 out of 4 patients. This contrasts with the majority of existing literature, which suggests a risk of SOTr as IMIDs induce T-cell proliferation, IL-2 & IFN-γ production & inhibit regulatory T-cell function. As all of our patients were concurrently on an anti-CD38 antibody, it raises a hypothesis about daratumumab potentially mitigating the risk of rejection. A recent study demonstrated that anti-CD38 Felzartamab was effective in the treatment of antibody mediated rejection, & while T-cell mediated rejection (TCMR) has been primarily associated with IMiD use, in this study, the anti-CD38 did not induce TCMR.
Additional studies exploring optimal IS strategies & the potential role of daratumumab in mitigating rejection risk for SOT patients on IMiD therapy are needed.