
Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
Category: Treatment of Relapsed/Refractory Myeloma (excluding T-cell redirection therapy)
Real-World Use and Effectiveness of Venetoclax in Combination with Carfilzomib Plus Dexamethasone in t(11;14)-positive Relapsed/Refractory Multiple Myeloma: A Single-Center Retrospective Study
 photo")
Maria Kotsopoulou, MD (she/her/hers)
Director of Hematology Clinic & B.M.T.U.
Metaxa Anticancer Hospital
The t(11;14) translocation in multiple myeloma (MM) is associated with elevated BCL-2 expression, providing a strong biological rationale for the use of venetoclax, a BCL-2 inhibitor. As BCL-2 is an anti-apoptotic protein, inhibition of BCL-2 by venetoclax leads to the activation of apoptosis and induction of malignant plasma cell death.
While clinical trials have shown promising results for venetoclax in this molecular subgroup, real-world data remain limited.
Methods:
We retrospectively analyzed the outcomes of four patients with relapsed/refractory multiple myeloma (RRMM) harboring t(11;14), treated at our institution with a combination of venetoclax, carfilzomib, and dexamethasone (VenKd).
All patients were triple-refractory to proteasome inhibitors (PIs), immunomodulatory drugs (IMiDs), and anti-CD38 monoclonal antibodies, with a median of three prior lines of therapy (range: 2–5). Three out of four patients (75%) had previously undergone autologous stem cell transplantation (ASCT), and 75% had additional high-risk cytogenetic features.
Data on treatment duration, response, and progression-free survival (PFS) were collected.
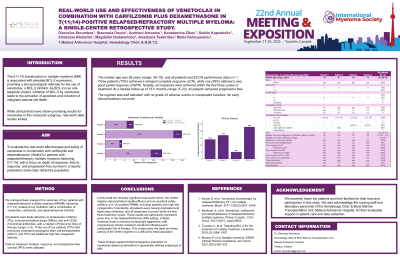
Results: The median age was 69 years (range: 58–78), and all patients had ECOG performance status 0–1. Three patients (75%) achieved a stringent complete response (sCR), while one (25%) attained a very good partial response (VGPR). Notably, all responses were achieved within the first three cycles of treatment. At a median follow-up of 15.5 months (range: 5–23), all patients remained progression-free.
The regimen was well tolerated, with no grade ≥3 adverse events or unexpected toxicities. No early discontinuations occurred.
Conclusions:
In this small but clinically significant real-world cohort, the VenKd regimen demonstrated notable efficacy and an excellent safety profile in t(11;14)-positive RRMM, including patients with high-risk cytogenetics. Importantly, all patients were heavily pretreated and triple-class refractory, and all responses occurred within the first three treatment cycles. These results are particularly impressive given that, in the relapsed/refractory (RR) setting, multiple myeloma tends to become increasingly aggressive, with progressively shorter remission durations following each subsequent line of therapy. This underscores the rapid and deep activity of the VenKd regimen in a difficult-to-treat population.
These findings support further prospective evaluation of venetoclax-based combinations in genetically defined subgroups of MM.